|
Zeiss IOLMaster Customer Service: 1-877-486-7473 ext.
4030
IOLMaster — Silicone
Oil.
Silicone oil is sometimes temporarily placed in the vitreous cavity for recurrent retinal detachments in eyes with proliferative
vitreoretinopathy, proliferative diabetic retinopathy, cytomegalovirus retinitis, giant retinal tears, and following perforating injuries. Axial length measurements by ultrasound of an eye in which the vitreous cavity has been filled with silicone oil is an exercise with many potential pitfalls, especially
if the silicone oil has become emulsified.
There are presently two viscosities of silicone oil in use:
-
1,000 mPa.s. silicone oil (Silikon, Alcon Laboratories, Ft. Worth, Texas) slows sound waves to a little more than half the speed (980 m/sec) of normal
vitreous and can attenuate the returning sound wave during ultrasonography so
much that a good echoes are difficult, if not impossible, to obtain.
-
5,000 mPa.s. silicone oil (ADATO SIL-ol 5000, Bausch & Lomb Surgical, San Dimas, California) has a somewhat higher density, and slows sound waves to
approximately 1,040 m/sec. Typically, when ultrasound measurements are
made through silicone oil, hugely erroneous axial lengths (such as 35 mm)
are displayed.
Until the introduction of partial coherence interferometry with the
Zeiss IOL Master, accurate ultrasound measurements of the axial length of
the human eye with silicone oil in place were difficult and complex. Each
component of the eye had to be individually measured (usually at 1,532
m/sec) and the true axial length calculated using the velocity
conversion equation (TAL = Vc / Vm x AAL) for the lens thickness and the vitreous cavity.
 In contrast, using partial coherence interferometry to measure eyes containing silicone oil in the vitreous cavity with the IOL Master is
relatively easy: In contrast, using partial coherence interferometry to measure eyes containing silicone oil in the vitreous cavity with the IOL Master is
relatively easy:
What was once a time-consuming, difficult and sometimes inaccurate measurement by ultrasonography is now simple and highly reproducible.
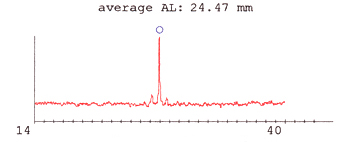
Phakic axial length measurement of an eye
with
the vitreous cavity filled with silicone oil.
As long as
the patient can see well enough to look directly at the
small, red, fixation light, the measurement will be to the center of the
macula, giving the refractive, rather than the axial length. This is
especially important for eyes that have posterior staphyloma.
If an IOL Master is not available, the next best approach would be,
prior to IOL placement, have the retina specialist first remove the silicone
oil. The axial length is then measured in the usual way and intraocular lens
power can then be calculated.
Adjustments to Intraocular Lens Power
If the silicone oil is to remain in the eye for an extended period of
time after cataract surgery, an adjustment to intraocular lens power must
be made.
Holladay, and others, have recommended that biconvex intraocular
lenses should not be placed in patients who have silicone oil in the vitreous
cavity. Instead, these patients should have a PMMA convex-plano lens,
with the plano side oriented so it is facing towards the vitreous cavity
and preferably over an intact posterior capsule. This approach prevents
the silicone oil from altering the refractive power of the posterior
surface of the intraocular lens. By contrast, a +20.00 diopter biconvex
intraocular lens could loose between a third and half of its refractive power if
it comes into contact with silicone oil. PMMA lenses are a first choice,
and silicone lenses should be avoided. The Holladay IOL
Consultant is very helpful for these cases as it is able to automatically compensate for the higher index of refraction of silicone oil in the vitreous cavity when doing these special IOL power calculations.
The additional power that must be added to the original IOL
calculation for a convex-plano IOL (with the plano side facing towards the
vitreous cavity) is determined by the following relationship, as described
in 1995 by Patel and confirmed by Meldrum:
-
Ns = refractive index of silicone oil (1.4034).
-
Nv = refractive index of vitreous (1.336).
-
AL = axial length in mm.
-
ACD = anterior chamber depth in mm.
Additional IOL power (diopters) = ((Ns - Nv) / (AL - ACD)) x 1,000
For an eye of average dimensions, and with the vitreous cavity filled
with silicone oil, the additional power needed for a convex-plano PMMA
intraocular lens is typically between +3.0 D to +3.5 D.
For more information on this topic, the following references are
helpful:
1. Axial Eye Length Measurements (A-Scan Biometry) in Byrne SF, Green
RL
(eds): Ultrasound of the Eye and Orbit. St. Louis, Mosby, Second
Edition,
2002.
2. Byrne SF: A-scan Axial Length Measurements - A Handbook for IOL
Calculations. Mars Hill, Grove Park Publishers, 1995.
3. Hoffer KJ: Ultrasound velocities for axial length measurement. J
Cataract Refract Surg 1994; 20: 554.
|