Aged-related Macular Degeneration (ARMD).
We invite you to make an appointment and learn more: 480-981-6111.
Home Test for Macular Degeneration:
We have provided a printable Amsler
grid for
you. Patients can help monitor their vision regularly and can detect distortions
in vision. These distortions represent the earliest stages of wet macular
degeneration.
Regardless of the treatment therapy followed, patients
with advanced dry macular degeneration should check the vision in each
eye, one at a time, at least once a day by staring at the central point
on an Amsler
grid.
Macular Degeneration.
If you have been diagnosed with macular degeneration you are in very
good company. In the United States alone, a new case is diagnosed every
three minutes, affecting:
-
One in six Americans between the ages of 55 and 64
-
One in four between the ages of 64 and 74
-
One in three over the age of 75
Although it almost never causes total blindness, macular degeneration is theleading
cause of vision loss in people over 50 in our country. Therefore, it is importantthat
you work with your doctor to learn to identify the problem early in an attemptto
keep the development of macular degeneration from getting worse or to slow it
down.

TOP
How Macular Degeneration Works
| |
 |
| |
Macular degeneration
affects central vision.
|
| |

|
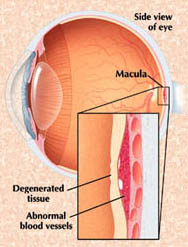
Macular degeneration is a disease caused by damage to or the breakdown of the macula, a tiny oval area in the retina, where the photoreceptors are most dense and where incoming images are focused.
The center of the macula is called the fovea and is responsible for
fine detail vision - our central (or reading) vision, both for distance and
close up. When the eye is directed at an object to be seen, whichever part
is focused on the fovea will be the clearest, the most in-focus image seen.
So, your ability to see fine centralized detail is directly dependent upon
the condition of the macula and fovea.
In macular degeneration, something goes wrong with the macula (as explained in
more detail below) and it slowly stops working. When this happens, vision
fades in the middle (the fovea), usually leaving the peripheral, or
side vision. It is uncommon for someone with macular degeneration to lose both
macular (detail) and peripheral (side) vision, or to lose vision completely
in both eyes.
|
TOP
Types of Macular Degeneration
There are two forms of age-related macular degeneration:
Dry macular degeneration (Atrophic ARMD)
Wet macular degeneration (Choroidal Neovascularization
- CNV)
|
Dry Macular
Degeneration
The vast majority of cases of ARMD are the dry type, which always
precedes the wet type -- although it doesn't always turn into that. Dry
refers to the slow degenerative process that occurs in which the macula
forms yellow deposits, called drusen and then becomes
progressively thinner but does not leak, and so is considered 'dry'.
Progression of dry macular degeneration takes a very long time and
does not always affect both eyes equally. Most people usually maintain
some central vision in at least one eye.
|
|
Wet Macular Degeneration (CNV)
Wet ARMD always arises from pre-existing dry ARMD. This occurs in about
10 to 15% of people with advanced dry macular degeneration. Newly formed,
abnormal blood vessels grow underneath the retina in the area of the
macula. These vessels leak fluid, bleed, and lift up the retina. When
this happens central vision is reduced and is often distorted. Eventually,
scar-like tissue forms under the macula and the eye loses its ability
to see detail. If CNV occurs in one eye, there is an increased chance
it will occur in the other eye.
|
TOP
Symptoms of Macular Degeneration
There is no pain associated with dry or wet macular degeneration. Vision
loss usually occurs gradually and typically affects both eyes at different
rates. Sometimes only one eye loses vision while the other eye continues
to see well for years. If both eyes are affected, reading and close up work
can become quite difficult. Even with a loss of central vision, however,
peripheral vision may remain clear.
|
The condition may be hardly noticeable in its early stages. A very frequent
and important symptom to be aware of is distortion. Straight lines will not
look straight. A telephone pole or a doorframe may seem a little bent, crooked,
or irregular, as though seen through heat waves on a highway. An area of theAmsler
grid will appear distorted and the small boxes in the area will vary in
shape and size. Also, you may see a dark gray spot similar to the aftereffect
caused by a flashbulb. There may be other changes in vision: you may notice
that the size of an object appears different for each eye or that colors
don't look the same for each eye. These changes in eyesight are important
symptoms and anyone who has these symptoms should make sure to see the eye
doctor promptly. Do
not assume you simple need a new pair of glasses. Make your appointment
right away.
TOP
Causes of Macular Degeneration
The root causes of macular degeneration are unknown. Women are at a slightly
higher risk than men. Caucasians are more likely to develop macular degeneration
than African-Americans.
The macular contains many highly active and sensitive photoreceptors that
require and consume a great deal of energy. Generating this energy requires
a constant, rich supply of oxygen, nutrients and ions. Consequently, the macula
has one of the highest volumes of blood flow through its supply vessels. Anything
that interferes with this necessary rich blood supply can cause the macula
to malfunction and possibly become diseased.
Smoking is one of those factors that can reduce this vital blood supply
by contributing to overall narrowing of the blood vessels and thickening of
the blood. A high-fat, high cholesterol diet can lead to fatty plaque deposition
in the macular vessels, also hampering blood flow. Nutritional deficiencies,
such as shortage of antioxidants, may increase the tendency for fatty deposits
to stick to blood vessel walls.
TOP
Diagnosis of Macular Degeneration
In order to determine if you have macular degeneration and what form, your
doctor will measure your vision and examine your eyes. By looking at the retina,
your doctor will be able to tell if there is an abnormality. If drusen are
found, you will want to schedule regular check-ups to make sure that no further
damage is occurring. It may be necessary that photographs of each macula be
taken to use for future comparison. The following are tests given to fully
diagnose ARMD:
- Visual acuity test: to measure vision at a distance and close up
- Dilated pupil examination: to see the inside of the eye with an ophthalmoscope to check for drusen.
- Amsler grid: a
pattern of straight horizontal and vertical lines (click
here for a printable Amsler grid and instructions for use). To the person
with ARMD, the lines appear wavy, distorted or missing or a black spot may appear
in the center of the grid.
- Optical Coherence Tomography (OCT): uses light waves to create
a contour map of the retina and can show areas of thickening or fluid accumulation.
- Fluorescein angiography: If your doctor finds an abnormality and
suspects CNV, this special test will be done to detect blood vessels that might
be leaking. During the test, a dye is injected into the arm and quickly travels
throughout the blood system to the eye. Photographs are taken of the eye, which
will later be used during laser treatment.
|
TOP
Treatments of Macular Degeneration
In the early stages of dry macular degeneration, regular eye check-ups,
attention to diet, in-home monitoring of vision and possibly nutritional
supplements may be all that is recommended.
Currently, treatments for macular degeneration are rapidly advancing and
changing as often as every three months. Various treatments are currently
available, but most of these treatments are directed at the early stages
of wet ARMD.
- Thermal laser photocoagulation of the abnormal blood vessels
is one treatment for wet ARMD. In some cases, laser treatment can be done
to prevent or lessen severe loss of eyesight if the CNV is discovered early
enough. However, only 15% of patients with wet ARMD are eligible for this
therapy, and in about 50% of those cases, the blood vessels continue to
grow. Overall, this means that laser photocoagulation is only helpful in
about 7-8% of patients with wet ARMD.
The usefulness of laser photocoagulation is limited because of the location
of the blood vessels, under the center of the macula. If these blood
vessels are treated with the hot laser, the center of the macula would
be burned and immediate vision loss would result.
For this reason, laser surgery is only indicated if the leaky blood vessels have
developed away from the fovea, the central part of the macula.
- Photodynamic therapy (PDT) A drug called verteporfin is injected
into your arm. It travels throughout the body, including the new blood
vessels in your eye. The drug tends to "stick" to the surface
of new blood vessels. Next, a light is shined into your eye for about 90
seconds. The light activates the drug. The activated drug destroys the
new blood vessels and leads to a slower rate of vision decline. Unlike
laser surgery, this drug does not destroy surrounding healthy tissue. Because
the drug is activated by light, you must avoid exposing your skin or eyes
to direct sunlight or bright indoor light for five days after treatment.
Photodynamic therapy is relatively painless. It takes about 20 minutes and can
be performed in a doctor's office.
Photodynamic therapy slows the rate of vision loss. It does not stop vision loss
or restore vision in eyes already damaged by advanced AMD. Treatment results
often are temporary. You may need to be treated again.
- Injections Wet AMD can now be treated with new drugs that
are injected into the eye (anti-VEGF therapy). Abnormally high levels of
a specific growth factor occur in eyes with wet AMD and promote the growth
of abnormal new blood vessels. This drug treatment blocks the effects of
the growth factor.
You will need multiple injections that may be given as often as monthly. The
eye is numbed before each injection. After the injection, you will remain
in the doctor's office for a while and your eye will be monitored. This
drug treatment can help slow down vision loss from AMD and in some cases
improve sight.
- Vitamins The National Eye Institute's Age-Related
Eye Disease Study (AREDS) found that taking a specific high-dose formulation
of antioxidants and zinc significantly reduces the risk of advanced AMD
and its associated vision loss. Slowing AMD's progression from the intermediate
stage to the advanced stage will save the vision of many people.
The specific daily amounts of antioxidants and zinc used by the study researchers were 500 milligrams of vitamin C, 400 International Units of vitamin E, 15 milligrams of beta-carotene (often labeled as equivalent to 25,000 International Units of vitamin A), 80 milligrams of zinc as zinc oxide, and two milligrams of copper as cupric oxide. Copper was added to the AREDS formulation containing zinc to prevent copper deficiency anemia, a condition associated with high levels of zinc intake.
People who are at high risk for developing advanced AMD should consider taking the formulation. You are at high risk for developing advanced AMD if you have either:
Intermediate AMD in one or both eyes.
OR
Advanced AMD (dry or wet) in one eye but
not the other eye.
Your ophthalmologist can tell you if you have AMD, its stage, and your risk for developing the advanced form.
The AREDS formulation is not a cure for AMD. It will not restore vision already lost from the disease. However, it may delay the onset of advanced AMD. It may help people who are at high risk for developing advanced AMD keep their vision.
- Low vision training may be the only truly effective option for the vast majority of patients. Whether it is vision loss for conditions such as ARMD, glaucoma or diabetes, low vision aids help patients perform normal activities of daily living and lead independent lives.
Low vision aids range from hand-held magnifying glasses to sophisticated systems that use video cameras to enlarge a printed page. Lifestyle aids such as large print books, tape-recorded books or magazines, large print playing cards, talking clocks and scales and many other devices are also available.
TOP Research on Macular Degeneration For those patients with wet ARMD, there is significant hope in the very near future. Ongoing clinical research is investigating new treatment strategies using photodynamic therapy. These studies are underway and the preliminary results are very encouraging. New drugs for macular degeneration:
One recent strategy that seems promising is a new class of drugs known as anti-angiogenic agents, which may stop the formation of blood vessels in wet ARMD and cause existing abnormal vessels to regress. The names of these drugs are rhuFab V2 (Genentech, Inc.), Macugen (Eyetech Pharmaceuticals) and Anecortave acetate (Alcon Research Ltd.). The preliminary results are encouraging, however these drugs are only available at this time to patients participating in a clinical study. New low vision device for macular degeneration:
For those patients who have already experienced vision loss and are somewhat stable, there is a new low vision device that is undergoing clinical investigation. This device is known as an intraocular miniature telescope (IMT) and is inserted into the eye at the time of cataract surgery. While this device may not help all patients with ARMD, there is a very good chance that the IMT could improve the ability to read and watch television. Genetic research on macular degeneration:
All treatments, so far, are designed to treat the vision loss associated with wet ARMD and slow the progression of the disease. None of the therapies really treat the underlying cause of ARMD. While the cause is still unknown, there is solid evidence that this is a disease with a strong genetic basis. For this reason, a great deal of research is going on to find the genes responsible for ARMD in the hope of someday developing a cure.
The eye specialists of East Valley Ophthalmology perform advanced
technology diagnostic testing and treatment, as well as taking
the time necessary to provide each patient with information needed
to fully understand their condition and to achieve their best possible
visual outcome.
If you would like further information, please call our office at:
480-981-6111
East Valley Ophthalmology
Eye Doctors - Mesa, ArizonaIf you or a family member
or friend have not had a recent routine eye examination, have a specific eye condition that needs addressing, or are looking for
an eye specialist or professional eye consultant please take a moment to Request an Appointment.
|