Acute angle-closure glaucoma is an emergency and should be treated immediately. Closed-angle glaucoma occurs when fluid cannot escape because the drainage angle is blocked, causing pressure to build up suddenly. This often causes noticeable pain.
Angle closure glaucoma is found much less frequently than open-angle glaucoma, but it can produce considerable vision loss in a short period of time. While there can be several causes of closed-angle glaucoma, it is most often caused by anatomical changes within the internal structures of the eye.
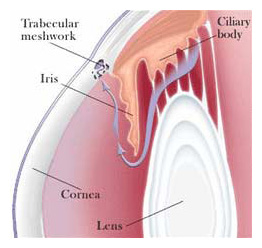
Acute closed-angle glaucoma is structurally different from open-angle glaucoma. With closed-angle glaucoma, the fluid in the eye cannot reach the drainage meshwork (trabecular meshwork) because clogging occurs before the meshwork. In contrast, with open-angle glaucoma, the clogging is within the drainage meshwork itself.
The trabecular meshwork is actually a tiny tissue filter that, if blocked by a change in size or shape of the tissue, will cause the intraocular pressure to elevate. In instances where the meshwork becomes blocked abruptly, it causes a sudden rise in intraocular pressure. This sudden rise in pressure can cause pain, redness, blurred vision, and, if left untreated, permanent loss of vision.
Closed-angle glaucoma is considerably more common in farsighted eyes, which tend to be smaller, and in patients between the ages of 45 and 60, where the crystalline lens is beginning to swell.
During your general eye exam, if your eye doctor observes or measures a narrowed angle, they will perform an additional examination procedure called Gonioscopy to fully visualize the meshwork and the angle, carefully assessing your predisposition to angle closure glaucoma. This test is performed by placing a special contact lens on the eye and then using the slit lamp biomicroscope to examine the meshwork and the angle thoroughly. If you are at risk for angle closure glaucoma, or if you have acute angle closure glaucoma, the most effective form of treatment is to use a laser to produce a small opening or hole in the iris so that aqueous humor can quickly and efficiently drain from the eye by preventing the trabecular meshwork from being blocked.