
Piggyback Lens Implantation?
When the calculated IOL power exceeds the available range, and placement of a single IOL would result in an unacceptable refractive outcome, one option is for the surgeon to place two IOLs in the eye during the same operative session. It is recommended that IOLs in different materials and locations be used to create a polypseudophakia lens pair. The previous practice of stacking two acrylic lenses in the capsular bag has since been abandoned due to occasional problems with interlenticular opacification and reduced visual acuity.
6 Steps for Polypseudophakia IOL Power Calculations:
When primary polypseudophakia is indicated, the IOL calculation is carried out in six logical steps, as follows:
Step 1
Measure the axial length as accurately as possible.
Even a relatively small axial length error in extreme axial hyperopia can result in a significant postoperative refractive error. The axial length in this setting is best measured using the Zeiss IOL Master. Immersion 10-MHz A-scan biometry is a reasonable alternative, albeit less accurate. The ACD and LT are typically measured using immersion biometry. The new Zeiss AC-Master will soon be available for this task, offering unprecedented accuracy of 0.001 mm.
Step 2
Calculate the total IOL power needed at the plane of the capsular bag.
For IOL power calculations in the setting of extreme hyperopia, the Holladay 2 formula is recommended. Hoffer Q, or a fully optimized version of the Haigis formula (a0, a1, and a2 optimized), is a reasonable alternative. Other 2-variable, third-generation theoretical formulas (such as SRK/T and Holladay 1) will typically require less IOL power than needed, resulting in postoperative hyperopia. This is because two-variable formulas are forced to make several assumptions as they estimate the effective lens position (ELPo), primarily based on keratometric central corneal power and axial length.
To begin, we must first calculate the total capsular bag IOL power. In primary polypseudophakia, the Alcon MA50BM, which has a negative shape factor (with the majority of IOL power on the posterior surface), is the preferred lens for the capsular bag. The design of this lens allows for the lowest possible profile at the level of the anterior lens capsule.

It is essential to ensure that the lens constant you will be using has been optimized. For axial lengths measured by the IOLMaster, it is possible to use something of a generic IOLMaster-adjusted Holladay 2 ACD of 5.55 mm for the MA50BM. We suggest that surgery for the non-dominant eye be performed first, targeting a refractive outcome of approximately -0.75 D. The IOL power for subsequent surgery on the dominant eye can then be fine-tuned using the refractive outcome of the first, non-dominant eye as a guide.
Step 3
Calculate the residual IOL power.
The highest power currently available for the MA50BM is +30.0 D. With this lens alone, we will come up short in terms of the total IOL power required.
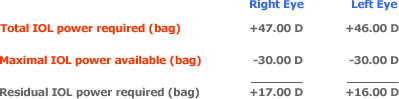
+17.00 D additional IOL power is required in the right eye and +16.00 D in the left eye to achieve the desired target refraction.
Step 4
Determine the power adjustment for the anterior (ciliary sulcus) lens.
Because of its more anterior position (closer to the principal plane of the cornea), an IOL at the level of the ciliary sulcus will have a greater effective power than if it were located at the level of the capsular bag. For this reason, the residual IOL power originally calculated for placement in the capsular bag will need to be adjusted.
The amount of power reduction required when moving an IOL from the capsular bag to the ciliary sulcus is proportional to the IOL power and can be determined by using the Refractive Vergence Formula as described by Holladay in his landmark 1997 Journal of Cataract and Refractive Surgery paper.
For primary polypseudophakia, a generalized estimation of this power reduction for modern biconvex IOLs is outlined below.
Note that this power reduction table differs from what would generally be expected in the setting of routine cataract surgery. This is because the ciliary sulcus IOL in primary polypseudophakia sits on top of the capsular bag IOL and is typically positioned slightly more anteriorly.

Step 5
Calculate the power of the anterior IOL.

The above provides us with the new power capabilities of the sulcus-placed IOL.
Step 6
Select the appropriate polypseudophakia lens pair.
It is recommended that different IOL materials be used in other locations to create a polypseudophakia lens pair.
For placement in the capsular bag, an IOL with a negative shape factor, such as the Alcon MA50BM, is an excellent choice because at +30.00 D, all but 1/5th of the lens power is located on the posterior surface. For the ciliary sulcus lens, a large diameter, low-profile, round-edge biconvex newer-generation silicone IOL, such as the Staar AQ-2010V (+5.00 D to +30.00 D) or the extended power range Staar AQ-5010V (-4.00 D to +4.00 D), is recommended.
This IOL combination lowers the likelihood of pigment dispersion, iris transillumination defects, intermittent uveitis, or secondary glaucoma, as well as the occasional “teeter tottering” of the sulcus-located IOL over a biconvex, or positive shape factor, capsular bag IOL. This also reduces the occurrence of interlenticular opacifications, which have all but disappeared following the abandonment of the original bag-in-bag acrylic combination.

The IOL strategy recommended for this patient is shown above. All should understand that, despite the very best and well-reasoned technique, the final postoperative refractive result may still differ from what is expected. And because extreme axial hyperopia is far outside anything that could be considered a normal range of operation for any IOL power calculation formula, deviations from expected are not uncommon. If this is the case, the silicone lens in the ciliary sulcus position can be exchanged for one of another power, leaving the higher power acrylic lens within the capsular bag.
In situations where the refractive outcome is not inevitable, the practice of operating on the non-dominant eye first is one additional way to fine-tune the refractive outcome when it comes time for surgery on the dominant eye. Dr. Joel Shugar in Perry, Florida, shared this approach with us many years ago, and we have found it very helpful when doing these very challenging IOL power calculations.
